Česká a slovenská psychiatrie

Časopis
Psychiatrické společnosti ČLS JEP
a Psychiatrickej spoločnosti SLS
původní práce / original article
- AKTUÁLNÍ ČÍSLO
- ARCHIV
- VYHLEDÁVÁNÍ
- PERIODIKUM
- REDAKČNÍ RADA
- PŘEDPLATNÉ
- INZERCE
- AKTUALIZOVANÉ
POKYNY
PRO AUTORY
- ISSN 1212-0383



- © Česká a Slovenská psychiatrie 2025
- © Galén 2025
ZMENY V KLINICKOM, FYZICKOM A PSYCHICKOM FUNGOVANÍ PRED A PO PANDÉMII COVID-19 U BIOLOGICKY LIEČENÝCH PACIENTOV S REUMATOIDNOU ARTRITÍDOU
CHANGES IN CLINICAL, PHYSICAL, AND PSYCHOLOGICAL FUNCTIONING BEFORE AND AFTER THE COVID-19 PANDEMIC IN BIOLOGIC-TREATED RHEUMATOID ARTHRITIS PATIENTS
Alexandra Husivargova Theofanidis1,2, Vladimira Timkova1, Zelmira Macejova3, Zuzana Kotradyova3, Dagmar Breznoscakova1, Robbert Sanderman2,4, Iveta Nagyova 1
1 Department of Social and Behavioural Medicine, Faculty of Medicine, PJ Safarik University in Kosice, Slovak Republic
2 Department of Health Psychology, University Medical Center Groningen, The Netherlands
3 1st Department of Internal Medicine, Faculty of Medicine, PJ Safarik University, Kosice, Slovakia and UNLP Kosice, Slovak Republic
4 Department of Health Psychology and Technology, University of Twente, Enschede, The Netherlands
2 Department of Health Psychology, University Medical Center Groningen, The Netherlands
3 1st Department of Internal Medicine, Faculty of Medicine, PJ Safarik University, Kosice, Slovakia and UNLP Kosice, Slovak Republic
4 Department of Health Psychology and Technology, University of Twente, Enschede, The Netherlands
SÚHRN
Husivargova Theofanidis A, Timkova V, Macejova Z, Kotradyova Z, Dagmar Breznoscakova D, Sanderma R, Nagyova I. Zmeny v klinickom, fyzickom a psychickom fungovaní pred a po pandémii COVID-19 u biologicky liečených pacientov s reumatoidnou artritídou
Cieľ: Krízové situácie, ako je pandémia COVID-19, môžu mať negatívny vplyv na fyzické a duševné zdravie, obzvlášť u pacientov s chronickými ochoreniami. Zamerali sme sa preto na skúmanie zmien v klinickom, fyzickom a psychickom fungovaní pred a po pandémii u biologicky liečených pacientov s reumatoidnou artritídou (RA).
Materiál a metódy: Vzorku tvorilo 103 pacientov s RA (81,6 % žien; priemerný vek 56,1 ? 13,8 rokov). Pacienti vyplnili General Anxiety Disorder Scale, Patient Health Questionnaire, 36-item Short Form Health Survey, Multidimensional Fatigue Inventory, a Visual Analogue Scale-pain. Na analýzu údajov sme použili t-test pre dva závislé výbery.
Výsledky: Naše výsledky preukázali výrazne zhoršenú bolesť a vyššiu úroveň anxiety po pandémii. Sociálne fungovanie a mentálny komponent kvality života sa naopak, v porovnaní s dátami pred pandémiou, signifikantne zlepšil. Naša analýza nepreukázala žiadne významné rozdiely medzi pred a post-pandemickými dátami pri depresii, fyzickom komponente kvality života, vo všeobecnej, fyzickej alebo mentálnej únave, či klinických premenných.
Záver: Naše zistenia naznačujú, že pandémia mala negatívny vplyv na pacientov s RA, a to najmä v oblasti zvýšenej úrovne bolesti a úzkosti. Naše zistenia indikujú, že okrem biologickej liečby môžu pacienti profitovať aj z nefarmakologických intervencií zameraných na problémy pretrvávajúce napriek farmakologickej liečbe, napríklad formou eHealth aplikácií, ktoré boli počas pandémie často používané.
Klíčová slova: anxieta, bolesť, COVID-19, fyzické zdravie, mentálne zdravie, pandémia, rheumatoidná artritída
ABSTRACT
Husivargova Theofanidis A, Timkova V, Macejova Z, Kotradyova Z, Dagmar Breznoscakova D, Sanderma R, Nagyova I. Changes in clinical, physical, and psychological functioning before and after the COVID-19 pandemic in biologic-treated rheumatoid arthritis patients
Objective: Crisis situations such as the COVID-19 pandemic can have a negative impact on people´s physical and mental health. We aimed to determine changes in clinical, physical, and psychological functioning before and after the pandemic in biologic-treated Rheumatoid Arthritis (RA) patients.
Methods: We included 103 RA patients (81.6% females; mean age 56.1?13.8 years). Patients completed the General Anxiety Disorder Scale, the Patient Health Questionnaire, the 36-item Short Form Health Survey, the Multidimensional Fatigue Inventory, and the Visual Analogue Scale-pain. Paired sample t-tests were used to analyze the data.
Results: Our results showed significantly worsened pain, and higher anxiety levels post-pandemic. In contrast, social functioning and mental component summary improved compared to pre-pandemic. Our analysis did not show any significant differences between pre- and post-pandemic outcomes in depression, physical component summary, general, physical or mental fatigue, and clinical variables.
Conclusions: Our findings suggest that the pandemic may have had a negative impact on patients with RA, as they were found to experience higher levels of pain and anxiety. In addition to their biological treatment patients may benefit from non-pharmacological interventions focused on prevalent problems, such as eHealth applications that were widely used during the pandemic.
Key words: anxiety, COVID-19, mental health, pain, pandemic, physical health, rheumatoid arthritis
INTRODUCTION
Rheumatoid arthritis (RA) is a chronic, systemic autoimmune connective tissue disease of unknown etiology, that leads to disability and premature death.1 With a global prevalence of 0.4-1.3%, the disease frequently manifests in middle age and in female patients (75%).2 Given the progressive course and incurability of RA, treatment aims to achieve clinical remission of symptoms using synthetic disease-modifying antirheumatic drugs (DMARDs), or if DMARDs are ineffective, using targeted synthetic DMARDs (tsDMARDs) or biologic response modifiers (bDMARDs).3 Considering their autoimmune condition, comorbidities, and use of immunosuppressive therapies, RA patients are a vulnerable group and may be more affected by infectious diseases, including Coronavirus disease 2019 (COVID-19).1,4
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), also known as COVID-19, broke out at the end of 2019 and rapidly swept across the globe. In March 2020 the World Health Organization (WHO) proclaimed it a pandemic and a major global health threat.5 To reduce disease spread, several preventive measures, including social isolation, were implemented around the world.5 Social isolation bestowed by lockdowns, quarantines, and curfews seriously constrained the access of people with chronic diseases, including RA patients, to medical care and medicines, which contributed to disease flare-ups.5-8 In the study by Fernandez-Avila et al. (2022), more than half of rheumatic patients self-reported psychological distress caused by social isolation.5
During lockdowns, most people did not have access to physiotherapy or exercise, 9 and physical activity in general was found to decrease, which might have enhanced the pain in RA patients.10 Pain levels also increased due to worsening clinical status as well as higher disease activity in patients, due to lower treatment adherence.11 The COVID-19 pandemic also had a significant negative impact on mental health, especially in patients with autoimmune diseases, such as RA.4,7 Depression and anxiety were frequently observed in RA patients even before the pandemic; furthermore, in crisis situations, fear enhances anxiety and stress levels in healthy people while exacerbating symptoms in those with pre-existing psychological distress.6 According to a recent study by Tee et al. (2020), anxiety and depression were higher in RA patients compared to the general population during the pandemic. The COVID-19 pandemic had a moderate or severe negative psychological impact on RA patients, with moderate to extremely severe anxiety identified in 38.7% of patients and depression in 27.7% of patients.6 In a study by Araujo et al. (2021) 67.3% of RA patients reported anxiety or that their pre-existing anxiety symptoms worsened, and more than 50% of patients reported newly developed or increased depressive symptomatology.10 Depression is not only a common comorbidity of RA, but it may be also a risk factor for physical disorders, such as RA or cardiovascular diseases,12,13 and it typically changes behaviour - reduction in physical activity, increased smoking, and dietary changes,12 all of which were recorded during the pandemic.14
Given that RA patients are a vulnerable population due to their autoimmune condition, comorbidities, and use of immunosuppressive therapies,1,4 more negative effects in their health-related quality of life (QoL) and increased protective behavior may be anticipated.5,14 The COVID-19 pandemic´s long-term effects on physical and mental health in RA patients are difficult to establish. However, studies have shown that people with chronic conditions may better cope with stressful events, as they are more resilient to managing physical limitations and psychological distress in the long term compared to the healthy control group.15,16 Therefore, we aimed to compare RA patients´ health outcomes before and after the pandemic to determine the changes caused by the outbreak and COVID-19-related measures, such as lockdowns, restrictions, quarantine, and social distancing, in biologic-treated RA patients.
METHODS SECTION
Sample and procedure
Participants in the study were recruited from a Rheumatology outpatient clinic in Kosice, Slovakia, that specializes in biological treatment. Enrollment required being RA diagnosed according to the American College of Rheumatology criteria17 and treatment with bDMARDs. Being under the age of 18 and being unable to communicate in Slovak were both exclusion criteria. Patients with comorbidities were not excluded from participating in the study.
Patients were enrolled for pre-pandemic data collection between April 2019 and February 2020. The postpandemic data collection lasted from March to December 2022. Patients in both collections received invitation letters, written informed consent forms, and self-report questionnaires in the mail, prior to their rheumatologist visits. Clinical data were collected during a rheumatological examination. Out of 156 patients approached, 103 agreed to participate (response rate 66%), 51 refused and 2 patients died. There were no significant differences in age, sex, or disease duration between responders and nonresponders.
The ethics committee of the Faculty of Medicine at PJ Safarik University in Kosice approved the study (No. 115/2011, 2021/EK/01001). All patients signed an informed consent form before participating in the study. Participation in the study was voluntary, with no incentives provided. The research follows Good Clinical Practice standards and the Declaration of Helsinki.
Measures
Health-related quality of life
The 36-Item Short Form Health Survey (SF-36) assesses health-related QoL. The SF-36 includes multi-item scales to measure eight subscales which create two components summary. Each total score can range from 0 to 100, with a higher score indicating better QoL.18 In our study, Cronbach´s alpha was 0.82 for social functioning, and 0.93 for the physical and mental component summaries.
Anxiety
Anxiety was measured using the General Anxiety Disorder Questionnaire (GAD-7). The total score on this 7-item self-report scale ranges from 0 to 21, with higher scores indicating higher levels of anxiety. The cut-off values for mild, moderate, and severe anxiety symptoms are 5, 10, and 15, respectively.19 Cronbach´s alpha in our sample yielded 0.89.
Depression
To assess depression the 9-item self-report Patient Health Questionnaire (PHQ-9) was used. It is designed to determine the presence of depressive symptoms based on the 9 DSM-IV criteria for a major depressive disorder. A four-point Likert scale is used to rate each item, with scores ranging from 0 to 27 and higher scores indicating greater depression. The cut-off scores for mild, moderate, moderately severe, and severe depressive symptoms are 5, 10, 15, and 20, respectively.20 Cronbach´s alpha in our sample yielded 0.85.
Fatigue
The 20-item Multidimensional Fatigue Inventory (MFI-20) was used to measure general, physical, and mental fatigue. Each subscale was assessed by four items scored on a five-point Likert scale, with higher scores indicating greater fatigue.21 In the present study, we used general, physical, and mental fatigue scores with Cronbach?s alpha calculated for each subscale being 0.80, 0.80, and 0.74.
Pain
The severity of the pain was assessed using a 100mm Visual Analogue Scale (VAS) , with scores ranging from 0 to 100, with a higher score representing greater pain.22
Clinical and sociodemographic variables
A rheumatologist assessed clinical variables, including disease activity and functional disability, during a patient visit. Additional data about the disease´s duration and sociodemographic variables such as age and sex were obtained from the patients´ medical records.
Disease activity was assessed using the Erythrocyte Sedimentation Rate (ESR) measured during the first hour (mm/1st hour), with a cut-off of 2-5 mm for males and 3-8 mm for females.23 The Disease Activity Score (DAS28) includes a tender and swollen joint count of 28, ESR, and a general health assessment on a visual analogue scale. The level of RA disease activity can be interpreted as remission (<2.6), low disease activity (2.6 to <3.2), moderate (3.3 to <5.1) , or high activity (>5.1).24
Functional disability was measured using the Health Assessment Questionnaire-Disability Index (HAQ-DI). This 20-item self-reported questionnaire evaluates fine movements of the upper extremities, locomotor activities of the lower extremities, and activities that involve both the upper and lower extremities in eight categories. A total HAQ-DI score from 0 to 1 represents "mild to moderate difficulty"; a score of 1 to 2 represents "moderate to severe disability", and 2 to 3 indicates "severe to very severe disability".25,26 Cronbach´s alpha in our sample yielded 0.87.
Statistical analyses
The descriptive statistics were performed first. Then we compared variables before and after the COVID-19 pandemic lockdowns, using a paired sample t-test. The data met the criteria for a normal distribution; therefore, only parametric statistics were used. The analyses were performed using the Statistical Package for the Social Sciences (IBM SPSS 25). Results were considered significant at p<0.05.
RESULTS
Sample characteristics
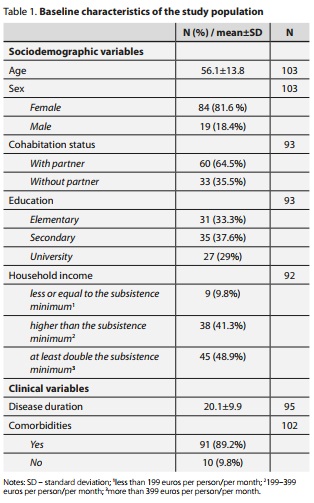
The study included 103 RA patients (81.6% female; mean age 56.1?13.8 years; disease duration 20.1?9.9 years). The majority of patients live in cohabitation with their partners (64.5%). Secondary education was identified as the most common (37.6%), then elementary (33.3%), and lastly university education (29%). The largest percentage of reported household income was at least double the subsistence minimum (48.9%), followed by income higher than the subsistence minimum (41.3%) and income less than or equal to the subsistence minimum (9.8%). Comorbidities were highly prevalent in our RA patients (89.2%) (Table 1).
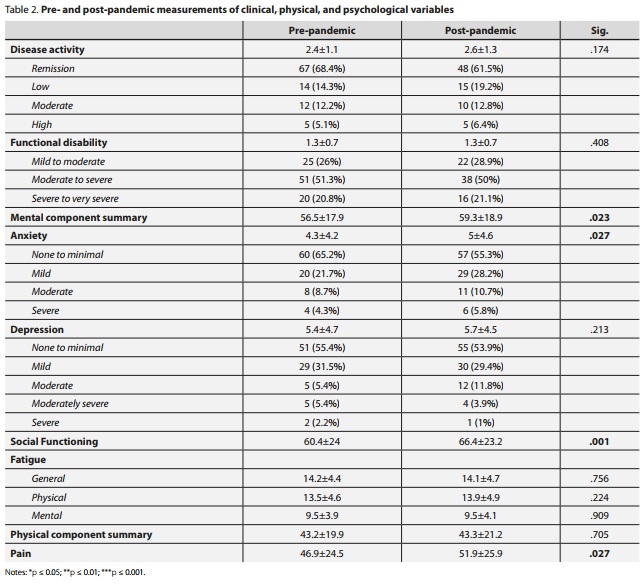
Pre- and post-pandemic comparison of the clinical, psychological, and physical variables in our sample
The majority of patients (68.4% pre-pandemic vs 61.5% post-pandemic) were in remission, followed by low disease activity (14.3.% pre-pandemic vs 19.2% post-pandemic). Half of the RA patients (51.3% pre-pandemic vs 50% postpandemic) experienced moderate to severe functional disability. There were no significant differences in disease activity or functional disability pre- vs post-pandemic in our sample. The mental component summary was found to be significantly better (p<0.05) in post-pandemic data collection. Also, social functioning significantly improved after the pandemic (p<0.001). Anxiety showed a small but significant (p<0.05) increase in post-pandemic measurements. A significant difference (p<0.05) was reported in the level of experienced pain before and after the pandemic, with higher pain identified after the pandemic. Depression, general, physical, together with mental fatigue, and physical component summary were not significantly different when compared to pre- and post-pandemic data.
DISCUSSION
This study aimed to compare RA patients´ health outcomes before and after the COVID-19 pandemic to determine the changes caused by the virus outbreak and COVID-19-related measures. We found that patients reported significantly higher levels of anxiety and pain, but better mental component summary and social functioning. No significant differences were found in depression, fatigue, physical component summary, or clinical variables before and after the pandemic.
We found significantly better mental component summary reported by patients after the pandemic compared to the pre-pandemic era. Studies found that RA patients were more resilient to stress than control participants during the pandemic, most likely because people without chronic conditions are less used to dealing with physical and mental discomfort and the resulting uncertainty.15,16 The resilience of RA patients is formed through a dynamic process of learning in response to various challenges; this does not mean that they do not experience stress; however, they do understand how to cope with suffering and difficulties and find a way to deal with the situation.15
Despite improvement in mental component summary score, significantly higher levels of anxiety in RA patients were reported in our sample. The explanation may lay in the SF-36 questionnaire, which has been identified as a poor predictor of anxiety.27 Our finding of increased anxiety is in line with the findings of the European League Against Rheumatism (EULAR) during the pandemic.28 The study by Itaya et al. (2021) found higher levels of anxiety during the pandemic, which was associated with higher disability scores and bDMARDs treatment.29 Because RA patients are at a greater infection risk than the general population, they may be worried about COVID-194,30 and they may be more likely to suffer from fear and anxiety as a result of it.31 Furthermore, the unsettling nature of information about the potential risks of rheumatic drugs against COVID-19 might have enhanced psychological distress.29,30 In some countries, a shortage of pharmacological treatment was reported,5,6,32 which could put RA patients under added pressure given their dependence on medication. Additionally, the pandemic caused economic problems and job insecurity,31 putting many RA patients with physical disabilities and coexisting comorbidities in a vulnerable position, which may have a negative impact on mental health.5,7 It was also reported that patients´ anxiety grew with each successive wave of COVID-19 within the first year.33 Another explanation for the high anxiety level in our RA patients is the Russian invasion of Ukraine that began in February 2022. The invasion may have alarming implications for global mental health, affecting not only Ukrainians but also communities worldwide,34-36 especially neighbouring countries, such as Slovakia or Poland, where citizens experience fear from this uncertain situation.37,38
The depression measured by the PHQ-9 scale showed no significant difference before and after the pandemic in our sample. However, more than half of our patients reported no to having minimal depression symptoms, with only 13% reporting moderate to severe depression. Similarly, Itaya et al. (2021) observed that higher levels of depression were not found after COVID-19 broke out, and depression was associated only with previously reported depression.29 In a Canadian study, patients with a history of mood disorders were identified as being more than twice as likely to report depression, which peaked early in the pandemic.33 Additionally, RA patients with higher disease activity were previously found to have reported more severe depression;7 meanwhile, in our sample, 82.7% of the patients were in remission or had low disease activity.
In contrast to the COVID-19 outbreak and its peak, when it was generally reported that the pandemic caused a loss of social function39 and rheumatic patients were more committed to strict isolation,14,15 our sample reported significantly better social functioning following the pandemic. A Danish study also found that rheumatoid patients were more self-isolated even after the gradual reopening, particularly working females treated with bD-MARDs.9 Even though our patients were all bDMARDs treated, with a high number of comorbidities (90.3%), predominantly females (81.6%), and 40.8% of patients were employed, we did not confirm the results of the Danish study. On the contrary, in our study male, but especially female patients reported their social functioning as significantly better than before the pandemic, which may have been caused by the time of our data collection which was conducted two years after the pandemic outbreak. Thus, patients may be less concerned about COVID-19 infection and its consequences than at the beginning or during the peak of the pandemic, or they may feel relieved to be able to socialize again and appreciated it more. Patients may have been impacted by months of uncertainty and worry; so, social functioning after the pandemic, which is closer to pre-pandemic life, was rated higher as a result of the restrictions experienced. Moreover, a study by Ian-nuccelli et al. (2021) found that lockdowns in some cases reduced the daily hassles of families, such as taking children to different activities or reducing other responsibilities, which can be stressful for parents. They also reported having more free time as a result of lockdowns, so they had more time to improve parent-child bonding.15 Lesse et al. (2022) also reported that some patients expressed a new sense of collectiveness during the pandemic. They expressed a positive perception, particularly the feeling that "we are all in it together", "battling our challenges together", and the sense of caring and compassion when people describe encouraging stories from similar situations they have been in.40 However, during the pandemic, we encountered a widespread wave of misinformation via digital media and social networks, which had the potential to be especially harmful because it was the primary source of information for many people. According to Krajčovič, only 52% of Slovak Internet users were able to detect the hoaxes,41 so the rest of the population was prone to believing in fake news or conspiracies, which led to anti-vax movements, with only 31% of the Slovak population receiving a booster vaccination,42 and polarization in society - similar to other nearby post-soviet countries.43,44
Even though fatigue was reported as a new symptom during the pandemic in 18% of rheumatic patients,32 our sample did not show a significant change in pre- and postpandemic measurements. During the pandemic, some patients experienced increased fatigue, particularly those who had to multitask and balance their personal and professional responsibilities while staying at home, and it was hard to distinguish if the fatigue was RA-related or from the extra work.30 An interesting finding is that even though our patients reported better mental component summary after the pandemic than before, no significant improvement was seen in mental fatigue. Also, physical fatigue did not change significantly, and it remains an unmet issue for patients with a high occurrence, and non-pharmacological interventions focusing on fatigue in RA patients are needed.
When compared to other studies,10,30 our patients did not report a significant change in physical component summary, which may be due to the high prevalence of remission or low disease activity. Many patients around the world were afraid to go to their appointments out of concern that they would catch COVID-19,14 and some countries reported a shortage in treatment.4,6,40 In our sample, patients continued their treatment and had no difficulty obtaining bDMARDs, so their clinical status did not change significantly from before the pandemic. RA patients in a UK study reported worse physical health in those who were under stringent social distancing.45 Also, during the pandemic, many patients were unable to continue with rehabilitation exercises or a physiotherapy programme, and European rheumatic patients also reported an increase in unhealthy behaviors (alcohol consumption, increased smoking, and weight gain) that may have contributed to a perceived worsening of physical QoL.14 On the other hand, in a Canadian study, working from home led some RA patients to be more physically active, and made it easier for them to prepare healthier meals.40 Due to missing data during the lockdowns, evaluating how the pandemic affected our RA patients? physical health is difficult, but results show that patients? physical health during post-pandemic data collection was not significantly different than their health before the pandemic.
Levels of pain were reported to be higher after the pandemic compared to the pre-pandemic period. These results correspond with earlier research that also found higher levels of pain during the pandemic.14,30 Daily physical activity in normal circumstances has a significant effect on experienced pain, stiffness, and well-being,10,11 which was disturbed by lockdowns. Higher levels of pain are associated with more active disease,14 but in our study, the clinical status of patients was not significantly changed and over 80% of the patients were in remission or with low disease activity. However, the reported pain was higher, even with continuous bDAMRDs treatment; thus non-pharmacological interventions should be included in the management of RA to reduce pain, such as exercise or Cognitive Behavioural Therapy.46
We found that disease activity or functional disability did not change significantly in our sample of RA patients when compared to current studies from countries with reported deficits of RA medication.5,11 Thus, we may assume that the clinical status of our RA patients did not worsen as the continuity of care in our patients was maintained, with no change in accessibility of bDMARDs treatment.
Strengths and Limitations
The main strength of our study is the comparison of data collected before and after the pandemic in the same study sample. Another strength is the homogenous group of established RA patients undergoing biological treatment with the majority of the patients in remission or with low disease activity.
However, because the data was collected in a single center specializing in bDMARDs and our sample did not include early diagnosed patients, generalizing the findings is limited. Another limitation is the lack of data from the time of the outbreak and the peak of the pandemic. We also did not evaluate patients´ concerns about COVID-19, their living situation, or whether they worked from home during the pandemic, all of which could have an impact on some of the factors we measured. More male participants are required to establish sex differences. Finally, an ongoing Russian invasion of Ukraine that began a couple of days before the post-pandemic data collection could also have influenced our results. The hospital where the data were collected is about 100 kilometers away from the border, and some patients live even closer, just a few kilometers away from the war conflict; thus, watching the number of incoming refugees and war scenes on television or social media on a daily basis may have increased psychological distress.
Implications for practice and future research
Further research is needed to investigate how the pandemic affects mental and physical health in RA over the long term, along with an in-depth analysis of confounding variables (such as whether patients recovered from COVID-19 infection or suffered from multimorbidity) that could have had an impact on our findings. Identification of physical and psychological changes due to the COVID-19 pandemic may enhance the understanding of patients´ needs; thus, routine screening should be regularly performed to help patients with targeted non-pharmacological interventions, in person or via eHealth applications.8, 46 Future research should take into account diverse government regulations that vary by country, resulting in variability in healthcare access and routine disease management. Furthermore, RA patients are not a homogeneous group, and we must account for differences in before and after pandemic experiences based on socioeconomic status, ethnic background,47 living situation, employment, or parental status, as well as confounders related to different crises such as war conflict.
CONCLUSION
Research on the effects of the pandemic outbreak on psychological, physical, and clinical factors in rheumatic diseases is still limited, but it is increasing. Our results indicate that pharmacological treatment alone is insufficient in stressful times, such as a pandemic, due to worsening problems. Healthcare professionals who treat RA patients should pay close attention not only to physical symptoms, such as pain which is common and has increased significantly after the pandemic, but also to the presence of psychological distress. The increased number of studies about mental health problems is important due to both an underlying predisposition for these conditions caused by RA and the impact of the pandemic. Psychological distress has been previously identified to have a negative impact on the progression and outcomes of rheumatic diseases, emphasizing the importance of early detection and the development of effective non-pharmacological interventions. Therefore, it is crucial to make sure that the course of medical treatment includes psychological interventions, focused on worsening symptoms such as pain and anxiety, especially during the challenging phase of a crisis. Additionally, more eHealth applications and telemedicine were used during the pandemic, which may be feasible for RA patients´ self-management.
CONFLICT OF INTEREST
No potential conflict of interest was reported by the authors.
DATA AVAILABILITY STATEMENT
Pseudonymised data can be made available from the corresponding author upon reasonable request, and it´s contingent upon a data use agreement.
ACKNOWLEDGMENTS
The authors would like to thank the patients with RA from the Rheumatology outpatient department in Kosice, who participated in this study.
REFERENCES
- 1. Tanski W. The Role of Clinical Activity, Loneliness, and Satisfaction with e-Health Services as Factors Affecting Quality of Life in Patients with Rheumatoid Arthritis During the SARS-CoV-2 Pandemic. Psychology Research and Behavior Management 2021; 14: 1581-1590.
- 2. Latocha KM, Loppenthin KB, Ostergaard M, Jennum PJ, Christensen R, Hetland M et al. Cognitive behavioural therapy for insomnia in patients with rheumatoid arthritis: protocol for the randomised, single-blinded, parallel-group Sleep-RA trial. Trials 2020; 21 (1): 440.
- 3. Smolen J, Landewe RBM, Bergstra SA, Kerchbaumer A, Sepriano A, Aletaha D et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Annals of the Rheumatic Diseases 2022 (0): 1-16.
- 4. Gonzalez-Rangel J, Perez-Munoz B, Casillas-Santos D, Barrera-Vargas A, Vazquez-Cardenas P, Escamilla-Santiago R et al. Mental health in patients with rheumatic diseases related to COVID-19 pandemic: Experience in a tertiary care center in Latin America. Lupus 2021; 30 (12): 1879-1887.
- 5. Fernandez-Avila DG, Barahona-Correa J, Romero-Alvernia D, Kowalski S, Sapag A, Cachafeiro-Vilar A et al. Impact of COVID-19 pandemic on patients with rheumatic diseases in Latin America. Rheumatology International 2022; 42 (1): 41-49.
- 6. Tee CA, Salido EO, Reyes PWC, Ho RC, Tee ML. Psychological state and associated factors during the 2019 coronavirus disease (COVID-19) pandemic among Filipinos with rheumatoid arthritis or systemic lupus erythematosus. Open Access Rheumatology: Research and Reviews 2020; 12: 215222.
- 7. Hassan MS, Mostafa DI, Abdelhady EI, Sarhan SA, Abdelghani M, Seleem DA. Psychosocial and clinical impact of COVID-19 pandemic and its relationship to the quality of life in patients with rheumatoid arthritis: a cross-sectional study, Egypt. Middle East Current Psychiatry 2022; 29 (1): 16.
- 8. Havrillová D. Kvalita života onkologických pacientov počas pandémie Covid-19: prehľadová štúdia. Československá psychologie 2022; 66 (4): 383397.
- 9. Glintborg B, Jensen DV, Engel S, Terslev L, Jensen MP, Hendricks O et al. Self-protection strategies and health behaviour in patients with inflammatory rheumatic diseases during the COVID-19 pandemic: results and predictors in more than 12 000 patients with inflammatory rheumatic diseases followed in the Danish DAN-BIO registry. RMD open 2021; 7 (1): e001505.
- 10. Araújo FC, Goncalves NP, Mouräo AF. Impact of the mandatory confinement during the first wave of the SARS-CoV-2/COVID-19 pandemic in Portuguese patients with rheumatoid arthritis: results from the COVID in RA (COVIDRA) survey. Acta Reumatol Port 2021; 46 (2): 126-133.
- 11. López-Medina C, Ladehesa-Pineda L, Gómez-García I, Puche-Larrubia MÁ, Sequí-Sabater JM, Armenteros-Ortiz P et al. Treatment adherence during the COVID-19 pandemic and the impact of confinement on disease activity and emotional status: a survey in 644 rheumatic patients. Joint Bone Spine 2021; 88 (2): 105085.
- 12. Kitzlerová E, Anders M. Deprese a kardiovaskulární choroby - společný průnik na rovině psychosociální a behaviorální. Čes a slov Psychiat 2010; 106 (2): 87-92.
- 13. Romao VC, Fonseca JE. Etiology and Risk Factors for Rheumatoid Arthritis: A State-of-the-Art Review. Front Med (Lausanne) 2021; 8: 689698.
- 14. Garrido-Cumbrera M, Marzo-Ortega H, Christen L, Plazuelo-Ramos P, Webb D, Jacklin C et al. Assessment of impact of the COVID-19 pandemic from the perspective of patients with rheumatic and musculoskeletal diseases in Europe: results from the REUMAVID study (phase 1). RMD open 2021; 7 (1): e001546.
- 15. Iannuccelli C, Lucchino B, Gioia C, Dolcini G, Favretti M, Franculli D et al. Mental health and well-being during the COVID-19 pandemic: stress vulnerability, resilience and mood disturbances in fibromyalgia and rheumatoid arthritis. Clin Exp Rheumatol 2021; 39: 153-160.
- 16. Džuka J, Klučárová Z, Babinčák P. COVID-19 na Slovensku: ekonomické, sociálne a psychologické faktory subjektívnej pohody a symptómov depresie v čase pandémie. Československá psychologie 2021; 65 (2): 125-145.
- 17. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 1988; 31 (3): 315-324.
- 18. Ware JE, Sherbourne CD. The MOS 36-Item Short-Form Health Survey (SF-36). Medical Care 1992; 30 (6): 473-483.
- 19. Spitzer RL, Kroenke K, Williams JBW, Lowe B. A Brief Measure for Assessing Generalized Anxiety Disorder. Arch Intern Med 2006; 166 (10): 1092-1097.
- 20. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. Journal of General Internal Medicine 2001; 16 (9) : 606-613.
- 21. Smets E, Garssen B, Bonke Bd, De Haes J. The Multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. Journal of Psychosomatic Research 1995; 39 (3): 315-325.
- 22. Huskisson EC. Measurement of pain. Lancet 1974; 2: 1127-1131.
- 23. Javorka K. Lekárska fyziológia. Učebnica pre lekárske fakulty. Martin: Osveta 2001; 80-8063-023-2: 678.
- 24. Van der Heijde DM, Van´t Hof MA, Van Riel PL, Van Leeuwen MA, Van Rijswijk MH, Van de Putte LB. Validity of single variables and composite indices for measuring disease activity in rheumatoid arthritis. Annals of the Rheumatic Diseases 1992; 51 (2): 177-181.<(li>
- 25. Bruce B, Fries JF. The health assessment questionnaire (HAQ). Clinical and Experimental Rheumatology 2005; 23 (5): S14.
- 26. Szilasiova A, Macejova Z, Nagyova I, Kovarova M, Beresova A, Szilasiova J. Reliabity and Validity of the Slovak Version and Modification of the Stanford Health Assessment Questionnaire-Functional Disability Index (HAQ) in Patient with Rheumatoid Arthritis (RA). Vnitrni lekarstvi 2002; 48 (1): 8-16.
- 27. Silveira E, Taft C, Sundh V, Waern M, Palsson S, Steen B. Performance of the SF-36 health survey in screening for depressive and anxiety disorders in an elderly female Swedish population. Qual Life Res 2005; 14 (5): 1263-1274.
- 28. Landewé R, Machado PM, Kroon F, Bijlsma HW, Burmester GR, Carmona L et al. EULAR provisional recommendations for the management of rheumatic and musculoskeletal diseases in the context of SARS-CoV-2. Annals of the rheumatic diseases 2020; 79 (7): 851-858.
- 29. Itaya T, Torii M, Hashimoto M, Tanigawa K, Urai Y, Kinoshita A et al. Prevalence of anxiety and depression in patients with rheumatoid arthritis before and during the COVID-19 pandemic. Rheumatology 2021; 60 (4): 2023-2024.
- 30. Mancuso C, Duculan R, Jannat-Khah D, Barbhaiya M, Bass AR, Metha B. Rheumatic disease-related symptoms during the height of the COVID-19 pandemic. HSS Journal 2020; 16 (1): 36-44.
- 31. Sood S. Psychological effects of the Coronavirus disease-2019 pandemic. Research & Humanities in Medical Education 2020; 7 (11): 23-26.
- 32. Michaud K, Wipfler K, Shaw Y, Simon TA, Cornish A, England BR et al. Experiences of patients with rheumatic diseases in the United States during early days of the COVID-19 pandemic. ACR Open Rheumatology 2020; 2 (6): 335343.
- 33. Bartlett S, Schieir O, Valois MF, Boire G, Hazlewood G, Thorne C et al. More Than Half Of RA Patients With A Lifetime History Of Mood Disorders Were Anxious And Depressed During The Covid-19 Pandemic: Results From The Canadian Early Cohort (CATCH) Study. Annals of the Rheumatic Diseases 2022; 81: 204.
- 34. Riad A, Drobov A, Krobot M, Antalová N, Alkasaby MA, Peřina A et al. Mental Health Burden of the Russian-Ukrainian War 2022 (RUW-22): Anxiety and Depression Levels among Young Adults in Central Europe. International Journal of Environmental Research and Public Health 2022; 19 (14): 8418.
- 35. Koubova A, Kimhi S. Prediction of individual, community and societal resilience in the Czech Republic compared to Slovakia during the war in Ukraine. BMC Public Health 2024; 24 (1): 583.
- 36. Vargova L, Jozefiakova B, Lacny M, Adamkovic M. War-related stress scale. BMC Psychol 2024; 12 (1): 208.
- 37. Chudzicka-Czupala A, Hapon N, Chiang SK, Žywiolek-Szeja M, Karamushka L, Lee CT et al. Depression, anxiety and post-traumatic stress during the 2022 Russo-Ukrainian war, a comparison between populations in Poland, Ukraine, and Taiwan. Scientific Reports 2023; 13 (1): 3602.
- 38. Nowicka M, Jarczewska-Gerc E, Marszal-Wisniewska M. Response of Polish Psychiatric Patients to the Russian Invasion of Ukraine in February 2022 -Predictive Role of Risk Perception and Temperamental Traits. International Journal of Environmental Research and Public Health 2023; 20 (1): 325.
- 39. Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. General Psychiatry 2020; 33 (2): e100213.
- 40. Leese J, Backman CL, Ma JK, Koehn C, Hoens AM, English K et al. Experiences of self-care during the COVID-19 pandemic among individuals with rheumatoid arthritis: A qualitative study. Health Expectations 2022; 25 (2): 482-498.
- 41. Krajčovič P. The Media in Times of the Pandemic - Comparing Viewing Figures and Interactions of Serious, Tabloid and Conspiracy Media on Facebook During the Covid-19 Pandemic. Media Literacy and Academic Research 2022; 5 (2) : 212-224.
- 42. National Health Information Centre. COVID-19 - Kumulatívne počty zaočkovaných osôb 2023.
- 43. Butter M, Knight P. Covid Conspiracy Theories in Global Perspective New York: Taylor & Francis 2023.
- 44. Zhao SX, Chan KT, Colakoglu S, Zhang Q, Yan B, eds,. Comparative Studies on Pandemic Control Policies and the Resilience of Society. Singapore: Springer 2023; 181-200.
- 45. Cleaton N, Raizada S, Barkham N, Venkatachalam S, Sheeran T, Adizie T et al. COVID-19 prevalence and the impact on quality of life from stringent social distancing in a single large UK rheumatology centre. Annals of the Rheumatic Diseases 2021; 80 (6): 93.
- 46. Kozáková R, Bužgová R. Efekt kognitivně-behaviorální terapie u nemocných s chronickou bolestí. Čes a slov Psychiat 2023; 119 (2): 68-76.
- 47. Jánošová J. Psychický distres v inter-kultúrnych súvislostiach. Čes a slov Psychiat 2015; 111 (3): 148-154.